SBFT is often performed with a large volume (300-500mL) of barium to promote gastric emptying and optimally distend stomach,
duodenum and small bowel loops for proper barium filling and mucosal coating.
Occasionally,
water-soluble contrast will become the choice of contrast medium in SBFT examinations for patients with clinical suspicion for gastrointestinal perforation or post-surgical evaluation. A series of overhead abdominal radiographs were obtained at 15- to 45-minute intervals,
depending on the rate of barium progress in the small intestine until barium fills the right side of the colon.
Normal small bowel transit ranges from 30 to 120 minutes but it could be lengthened dramatically in patients with obstruction or adynamic ileus from various causes.
Assessment of the distribution,
course and size of each portion of small intestine is performed with fluoroscopic guidance and manual palpations are essential to separate individual small bowel loops and to identify abnormalities that might obscure by overlapping loops of small bowel.
When the barium suspensions reached the colon,
compression of the terminal ileum is essential for optimal visualization of this region,
which is usually obtained with the patient in a supine or a left posterior oblique position. Fig. 1b [1,2]
Anatomy
Gaining a good grasp of the SBFT examinations requires us to understand the distribution,
location,
and morphology of the small intestines.
Anatomically,
the small bowel can be divided into three parts; the duodenum,
jejunum and ileum.
The duodenum consists of four parts: first (superior),
second (descending),
third (horizontal),
and fourth (ascending) which run from the pylorus to the left upper quadrant and connected with the jejunum.
The length for duodenum is about 2-3m.
The mesenteric small intestine is divided into two part with the proximal 40% was known as jejunum and the distal 60% was made up by ileum.
Jejunum and ileum are small bowel loops in a pattern of a long convoluted tube with length for approximately 4-6-m.
[2] In SBFT,
the proximal jejunum lies in the left upper quadrant with a luminal diameter up to 3cm gradually tapers in diameter to the distal ileum with a luminal diameter up to 2cm lies in the right lower quadrant.
Fig. 1a [1] The surface area of the intestine is increased by the circumferential folds with the folds in the jejunum are higher,
thicker,
and more numerous (four to seven folds per inch) compare to the ileum (two to four folds per inch).[3]

Fig. 1: Normal small intestine. (A) Duodenum in the right upper quadrant consists of 4 parts: first (D1), second (D2), third (D3), and fourth (D4), which run from the pylorus to the left upper quadrant to connect with the jejunum (J) and the ileum (I) lies in the right lower quadrant. (B) Radiograph with compression shows the barium flow from the terminal ileum (T) to the cecum(C) through the ileocecal valve (V).
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan
An often overlooked segment in the SBFT
For an SBFT examination may be performed after a single-contrast upper gastrointestinal (UGI) series or as a separate study,
the UGI tract is sometimes not evaluated during SBFT examination. A survey conducted in year 2002 has shown that the UGI tract in SBFT study is not evaluated in a number of radiologic practices.[4] Moreover,
duodenum can easily be obscured by the stomach or other parts of small bowel in SBFT study,
which make it becomes an often overlooked segment in the SBFT examination.
Given the retroperitoneal position of the 3rd and 4th segment of the duodenum,
they often stay out of sight in the SBFT examination. Fig. 2 In recent radiology practice,
SBFT is no longer a specialized form of fluoroscopic examination for the evaluation of the mesenteric small intestine with the diverse clinical indications for this examination to be ordered. Most of the time,
pertinent symptoms such as abdominal pain,
diarrhoea,
vomiting and body weight loss that suspect a GI tract disease might serve as the clinical indications for the SBFT to be performed.[5] Consequently,
the upper gastrointestinal tract,
in particular,
duodenum,
should be also evaluated as part of the SBFT examination to optimize the diagnostic yield of this examination.

Fig. 2: Image in SBFT obtained at 15 minutes revealed the 2nd to 4th segments of the duodenum was totally obscured by the stomach.
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan
Interpretation of duodenum in SBFT
Like other parts of the small bowels,
the duodenum could be well evaluated in SBFT by analyzing the morphology of a focal lesion or the distribution,
location,
and morphology of the intestinal fold.
During fluoroscopic observation of the first pass of barium along the duodenum from the pylorus,
carefully delineating the duodenal sweep allows one to detect the abnormalities in the duodenum.
The position and location for each part of the duodenum and the duodenojejunal junction could be identified in the early filling of the duodenum or performed with the help of fluoroscopy to separate the overlying small bowels or stomach that obscured the duodenum with certain radiographic positioning. In this exhibit,
a miscellaneous collection of disease involving duodenum in SBFT study will be discussed.
Non-neoplastic duodenal disease
Intestinal Malrotation
Intestinal malrotation is defined by a congenital abnormal position of the bowel within the peritoneal cavity and usually involves both the small and the large bowel.
Through upper GI series or SBFT,
a diagnosis of intestine malrotation could be established,
but the subtype of the malrotation could only be determined by the latter examination.
The radiologist can distinguish malrotation from a normal position of the bowel by depicting the position of the duodenojejunal junction and the intestines.
Malrotation is determined when the duodenal-jejunal junction does not cross the midline and lies below the level of the duodenal bulb.
Malrotation comprises a range of malrotation types and classifications,
each reflecting the time at which a failure occurs during the embryologic rotation,
also known as intestinal nonrotation,
incomplete rotation or reverse rotation.
The non-rotation intestine is described as the small intestine distributed on the right and the colon at the left side.
Fig. 3 While the type of incomplete rotation is depicted as the nonrotation of small intestine with cecum lies in the midline,
the right upper quadrant or remains in a normal cecal position.
Reversed rotation is rare and it has been rotated in the clockwise direction during the embryologic rotation which depicted as a duodenum that rests anterior to the superior mesenteric artery and a transverse colon that is posterior to the superior mesenteric artery.
Intestinal malrotations are as a result of any variation in this rotation and fixation of the GI tract during development.
Therefore,
malrotation might result the malposition of the small bowel with the cecum remains in a normal location.
This normal location of the cecum may cause malrotation to be missed during interpretation of SBFT.[6] Fig. 4

Fig. 4: Incomplete rotation. (A) Image from a SBFT study at 15 minutes shows duodenum (D) connects to jejunum at the right upper quadrant with jejunum (J) lies over right side and ileum lie in the left side.(B) Following SBFT study of the same patient obtained at 90 minutes revealed barium flow from the ileum ( I ) to the cecum(C) in a normal position of the cecum ( arrow ).
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan

Fig. 3: Nonrotation of the bowel. A. Radiograph shows a low position of the duodenal–jejunal junction (arrow) below the duodenal bulb that fails to cross the midline with the small bowel located in the right side of the abdomen. B. The ileum connects to the cecum (arrow) and the colon which located primarily in the left side of the abdomen.
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan
Inflammatory process of duodenum
There is a wide spectrum of the cause and manifestation of the inflammatory process,
including intra-luminal or extra-luminal disease that can affect duodenum.
Inflammatory processes that often involve duodenum are owing to secondary involvement from inflammation of an adjacent organ,
malignancy,
or infectious process.
The most common inflammatory process to affect the duodenum is secondary involvement from pancreatitis and infectious process that caused by the Helicobacter pylori.[7] In SBFT,
inflammation that involved a certain part of the duodenum may be manifested by irregular tubular narrowing with thickened folds,
which frequently being recognized as inadequate luminal distention by barium or the barium has just passed through.
Fig. 5 Therefore,
evaluation with magnification view is essential whenever stricture or narrowing of the duodenum was detected in SBFT study.
Fig. 6 A definitive diagnosis of the inflammatory entity that involved the duodenum is made on the basis of laboratory evaluation and other testings as well as the clinical presentations and the result of physical examinations.

Fig. 5: Narrowing of the 2nd part of the duodenum was suspected in SBFT examination performed in a 15-year-old patient. This patient was diagnosed with eosinophilic duodenitis based on established clinical manifestations and histopathological findings.
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan

Fig. 6: Magnification view of the descending duodenum of the patient in Fig 5. (A and B). SBFT with barium revealed a pattern of irregular-segmental thickening and effaced fold with tubular narrowing (arrow) in descending duodenum, a “saw-tooth” appearance.
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan
Duodenal diverticula
Duodenal diverticula are protrusions of pouches or sacs from the mucosa of the duodenum through the muscular layers of the walls.
In SBFT,
duodenal diverticulum often detected as an incidental finding as most of the patients are asymptomatic.
The duodenal diverticula are commonly located on the medial border of the descending duodenum Fig. 7 near the ampulla of Vater, but it may also found in the third or fourth portion of the duodenum and the lateral border of the descending duodenum.
Fig. 8 Duodenal diverticula typically appear on SBFT as smooth,
round or ovoid outpouchings with a variety of size and shape arising on a discrete neck from the wall of the duodenum.
Detection of uncomplicated diverticulum should not be trivialized because the patients might experience duodenal diverticulitis,
which can be complicated by perforation or obstruction.[7]

Fig. 7: Duodenum diverticulum on the medial border of the descending duodenum. (A) A diverticulum in ovoid shape and smooth surface (arrow) was incidentally found in a 67-year-old patient during SBFT examination. (B) SBFT in another 33-year-old patient revealed a diverticulum with “mushroom-like" outpouching arising on a discrete neck from medial duodenum.
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan

Fig. 8: Duodenum diverticulum. (A) SBFT with barium in an 83-year-old patient showed an ovoid outpouching located on the lateral border of the descending duodenum (arrow). (B) A large outpouching arising on a discrete neck from the transverse duodenum (arrow) was detected during SBFT examination in a 59-year-old patient that presented with abdominal pain .
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan
Superior mesenteric artery (SMA) syndrome
SMA syndrome is characterized by vascular compression of the 3rd portion of duodenum related to loss of the intervening mesenteric fat pad between aorta and SMA.
The patient with SMA syndrome may present with unspecific chronic upper abdominal symptoms such as epigastric pain,
nausea,
postprandial discomfort,
early satiety,
and sometimes,
body weight loss. In SBFT or UGI barium study,
typical findings of SMA syndrome included extrinsic compression of a vertically oriented,
band-like defect on the 3rd portion of the duodenum,
dilatation of the proximal duodenum and stomach and delayed gastroduodenal emptying.
Radiological criteria at CT angiography are a reduction of the aortomesenteric angle to 22° or less (normal 25°–60°) and a decrease of the aortomesenteric distance to 8 mm or less (normal 10– 28 mm).[8] Fig. 9

Fig. 9: Superior mesenteric artery (SMA) syndrome. (A)SBFT at 45 minutes showed dilated duodenum proximal to an extrinsic impression of a band-like defect (arrow) on the third part of the duodenum. (B)Sagittal-reformatted CT shows an angle of 8.1 degrees between the SMA (arrowhead) and the aorta, with compression of the 3rd portion of the duodenum (arrow).
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan
Duodenal neoplastic process
A variety of tumours,
both malignant and benign,
may arise within the small intestine.
Neoplastic processes in the duodenum can be separated into benign and malignant pathogenesis.
Benign duodenal tumours may develop as a single lesion or as multiple lesions.
The most common benign neoplasm of the duodenum is an adenoma,
benign gastrointestinal stromal tumour (leiomyoma),
lipoma,
fibroma and various polyposis syndromes.
In SBFT,
benign duodenal tumour often illustrated as a solitary lesion,
multiple intraluminal filling defects with a smooth surface.
Malignant primary neoplasms of the duodenum are occasional.
Adenocarcinoma is the most common primary malignant neoplasm of the duodenum,
comprises for about 50%–70% of small bowel adenocarcinomas occurring either in the duodenum or proximal jejunum.[7] Other types of malignancy could be found in small intestine included neuroendocrine tumours (carcinoids),
stromal tumours,
and lymphomas.
Malignant duodenal mass lesions usually appear on SBFT as polypoid,
ulcerated,
or annular lesions that cause luminal narrowing and distortion of the normal surface pattern. Fig. 11 Although small bowel tumours are relatively rare,
primary neoplasms of the duodenum,
as well as a local extension from adjacent malignancies,
can be detected in SBFT. Careful scrutiny and attention to the duodenum can result in a reliable prospective diagnosis.

Fig. 10: Duodenal adenocarcinoma. (A)SBFT with barium showed dilatation of duodenum proximal to the 4th portion of the duodenum with irregular narrowing (arrow). (B)Subsequent abdominal CT revealed a low-density mass lesion (arrow) at the duodenal-jejunal junction which proved to be a duodenal adenocarcinoma.
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan
Intussusceptions
Intussusceptions of small bowels are rare entities with an invagination of a portion of the full thickness of the small bowel into the other part of the small bowel.
Gastroduodenal and duodenojejunal intussusceptions are usually associated with gastric or duodenal tumours that serve as the lead point.
The typical radiographic sign in barium study is coil spring appearance depicted by the intestinal mucosal fold of the intussuscipiens surrounding the intussusceptum.
Fig. 11 Abdominal CT might be helpful to discern the exact underlying disease of intussusceptions by identifying the presence of a lead point,
the configuration of the lead mass,
the degree of bowel wall oedema,
and the amount of invaginated mesenteric fat that affect the appearance of an intussusception.[9]
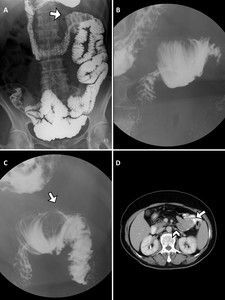
Fig. 11: Duodenojejunal intussusception in a 63-year-old patient with gastrointestinal bleeding and anemia. (A)Image from a SBFT study at 45 minutes shows a coil spring appearance at the duodenojejunal junction (arrow).(B)Spot radiograph of the duodenojejunal junction found that the duodenum with narrow lumen is telescoped into the jejunum. Barium coating of the intussuscipiens depicted the coil spring appearance.(C)A different view of spot radiograph detects a filling defect with a smooth surface within the lumen of the intussuscipiens(arrow).(D)Abdominal axial CT image of the same patient demonstrates an intussusception (arrowhead) and associated bowel wall thickening with a round soft-tissue mass(arrow) serving as a lead point. Pathologic evaluation revealed a gastrointestinal stromal tumour.
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan
Other patterns that suggest abnormalities
Extrinsic compression with displacement or widening of the duodenal sweep
Extrinsic compression of duodenum might suggest a variety of abnormalities that involved duodenum.
Dilatation of adjacent structures such as bile duct or vessels can also produce one or more extrinsic impressions on the outer wall of the duodenal bulb and sweep.
In detecting extrinsic compression of the duodenum by adjacent structures or extra-duodenal lesions in SBFT,
the contour of duodenum,
displacement or widening of the duodenal sweep could provide a clue to suspect an abnormality.
Abnormalities or diseases that often involve liver,
gallbladder,
colon,
right kidney and right adrenal gland may cause leftward displacement of the duodenal bulb and sweep.
Widening of the duodenal sweep with lateral displacement is always attributed to an abnormality arising from the medial side of the descending duodenum,
which highly suspected pancreatic head abnormalities.
Nonetheless,
numerous abnormalities including peritoneal fluid collection,
abscess formation,
various inflammatory or neoplastic processes of surrounding organs or tissues may compress,
displace,
or infiltrate the duodenum. Fig. 12 Fig. 13 Although displacement of the duodenal sweep with extrinsic compression could be easily recognized,
it is difficult to distinguish benign or malignant disease that displaced the duodenal sweep by SBFT examination.
Hence,
CT or other cross-sectional imaging studies should,
therefore,
be performed for a more definitive diagnosis.

Fig. 12: Peritoneal carcinomatosis with loculated fluid collection in a patient with ovarian cancer. (A)Image from a SBFT study shows extrinsic compression of the duodenum and lesser curvature with no mucosal abnormalities.(arrow)(B)Coronal reformatted contrast-enhanced CT image revealed peritoneal carcinomatosis (arrow) with the loculated fluid collection (*) in the same patient that caused the extrinsic compression on the lesser curvature and the duodenum(arrowhead).

Fig. 13: Cavitated lesion. (A)Image from a SBFT study shows widening of the duodenal sweep with lateral displacement and extrinsic compression of the transverse duodenum.(arrow)(B)Coronal contrast-enhanced CT image of the same patient revealed lateral displacement of the descending duodenum (arrowhead) by a cavitated mass lesion arising from the greater curvature.(arrow)
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan

 Duodenum in the right upper quadrant consists of 4 parts: first (D1), second (D2), third (D3), and fourth (D4), which run from the pylorus to the left upper quadrant to connect with the jejunum (J) and the ileum (I) lies in the right lower quadrant. (B) Radiograph with compression shows the barium flow from the terminal ileum (T) to the cecum(C) through the ileocecal valve (V).
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan")

 below the duodenal bulb that fails to cross the midline with the small bowel located in the right side of the abdomen. B. The ileum connects to the cecum (arrow) and the colon which located primarily in the left side of the abdomen. References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan")
 Image from a SBFT study at 15 minutes shows duodenum (D) connects to jejunum at the right upper quadrant with jejunum (J) lies over right side and ileum lie in the left side.(B) Following SBFT study of the same patient obtained at 90 minutes revealed barium flow from the ileum ( I ) to the cecum(C) in a normal position of the cecum ( arrow ).
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan")

. SBFT with barium revealed a pattern of irregular-segmental thickening and effaced fold with tubular narrowing (arrow) in descending duodenum, a “saw-tooth” appearance.
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan")
 A diverticulum in ovoid shape and smooth surface (arrow) was incidentally found in a 67-year-old patient during SBFT examination. (B) SBFT in another 33-year-old patient revealed a diverticulum with “mushroom-like" outpouching arising on a discrete neck from medial duodenum.
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan")
 SBFT with barium in an 83-year-old patient showed an ovoid outpouching located on the lateral border of the descending duodenum (arrow). (B) A large outpouching arising on a discrete neck from the transverse duodenum (arrow) was detected during SBFT examination in a 59-year-old patient that presented with abdominal pain .
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan")
 syndrome. (A)SBFT at 45 minutes showed dilated duodenum proximal to an extrinsic impression of a band-like defect (arrow) on the third part of the duodenum. (B)Sagittal-reformatted CT shows an angle of 8.1 degrees between the SMA (arrowhead) and the aorta, with compression of the 3rd portion of the duodenum (arrow). References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan")
SBFT with barium showed dilatation of duodenum proximal to the 4th portion of the duodenum with irregular narrowing (arrow). (B)Subsequent abdominal CT revealed a low-density mass lesion (arrow) at the duodenal-jejunal junction which proved to be a duodenal adenocarcinoma. References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan")
Image from a SBFT study at 45 minutes shows a coil spring appearance at the duodenojejunal junction (arrow).(B)Spot radiograph of the duodenojejunal junction found that the duodenum with narrow lumen is telescoped into the jejunum. Barium coating of the intussuscipiens depicted the coil spring appearance.(C)A different view of spot radiograph detects a filling defect with a smooth surface within the lumen of the intussuscipiens(arrow).(D)Abdominal axial CT image of the same patient demonstrates an intussusception (arrowhead) and associated bowel wall thickening with a round soft-tissue mass(arrow) serving as a lead point. Pathologic evaluation revealed a gastrointestinal stromal tumour.
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan")
Image from a SBFT study shows extrinsic compression of the duodenum and lesser curvature with no mucosal abnormalities.(arrow)(B)Coronal reformatted contrast-enhanced CT image revealed peritoneal carcinomatosis (arrow) with the loculated fluid collection (*) in the same patient that caused the extrinsic compression on the lesser curvature and the duodenum(arrowhead).")
Image from a SBFT study shows widening of the duodenal sweep with lateral displacement and extrinsic compression of the transverse duodenum.(arrow)(B)Coronal contrast-enhanced CT image of the same patient revealed lateral displacement of the descending duodenum (arrowhead) by a cavitated mass lesion arising from the greater curvature.(arrow)
References: Department of Medical Imaging, China Medical University Hospital - Taichung City/Taiwan")